

Translate this page into:
The accidental loss of guidewire during emergency femoral central venous cannulation: A case report

*Corresponding author: Sham Sunder Goyal, Department of Anaesthesiology and Intensive Care, Adesh Institute of Medical Sciences and Research (AIMSR), Bathinda - 151101, Punjab, India. shamgoyal_17@rediff.com
-
Received: ,
Accepted: ,
How to cite this article: Goyal SS , Panditrao MM, Garg A. The accidental loss of guidewire during emergency femoral central venous cannulation: A case report. Adesh Univ J Med Sci Res 2020;2(1):61-3.
Abstract
Many complications are reported with placement of the central venous catheter. They can be varied and graded as minor/insignificant, self-limiting, and not requiring any intervention to major/serious and requiring urgent intervention to save the life of the patient. Most of them can be minimized with certain precautions, use of aids and improved skill and experience of the operator. We are presenting a case report with such a complication, which is much rarer, happened, even in the hands of a very senior and experienced operator, requiring urgent intervention.
Keywords
Emergency central venous catheterization
Femoral approach
Guidewire
Accidental loss
Complication

INTRODUCTION
Central venous catheterization is one of the most common and routine procedures performed in any intensive care units (ICU), with an overall complication rate of 12%.[1] The experience of operator and advancement in the use of ultrasonography has reduced the central venous line placement complications.[2] The guidewire-related complications are cardiac dysrhythmias, conduction abnormalities, perforation of chambers or vessels kinking, loss, looping, breakage, and knot in guidewire.[3,4] The loss of a complete guidewire into the circulation is preventable and rare.[1] We report a case of complete loss of guidewire during femoral vein cannulation.
A 40-year-old male patient presented with 70% electrical deep burns (on anterior and posterior aspect of arms bilaterally, anterior and posterior aspect of chest, abdomen and back) in our ICU, who required emergency central venous access for the fluid resuscitation and antibiotics administration at the time of admission. At this time, patient was very agitated due to anxiety and severe pain and logically very uncooperative.
As there was no possibility of using the “usual” sites for the placement of central venous catheterization, due to the burns [Figure 1], the choice of the right femoral vein with the Seldinger technique was attempted by an experienced anesthesiologist (experience more than 10 years) posted in ICU. During cannulation, when only 3-4 cm of guidewire was left outside, probably due to an inadvertent body movements of the restless patient caused the guidewire to slip out of the anesthesiologist’s fingers following which, the negative intrathoracic pressure lead to sucking of guidewire into the circulation along with blood flow. An emergency iv Cannula 22 gauge was secured immediately on dorsum of foot with difficulty. The patient’s vitals were stable.

- Burns on entire trunk.
On radiography, the guidewire was seen to have ascended into inferior vena cava and entered the heart [Figure 2]. The migrated guidewire did not produce any cardiac complications to him. Patient was immediately shifted into the cardiac catheterization laboratory after consulting with cardiologist. The guidewire was then removed by cardiologist percutaneously using a gooseneck snare. The guidewire was grasped and removed uneventfully with a steady gentle pull under fluoroscopic guidance in the cardiac catheterization laboratory through left side approach [Figures 3 and 4]. The vitals were stable throughout the procedure.
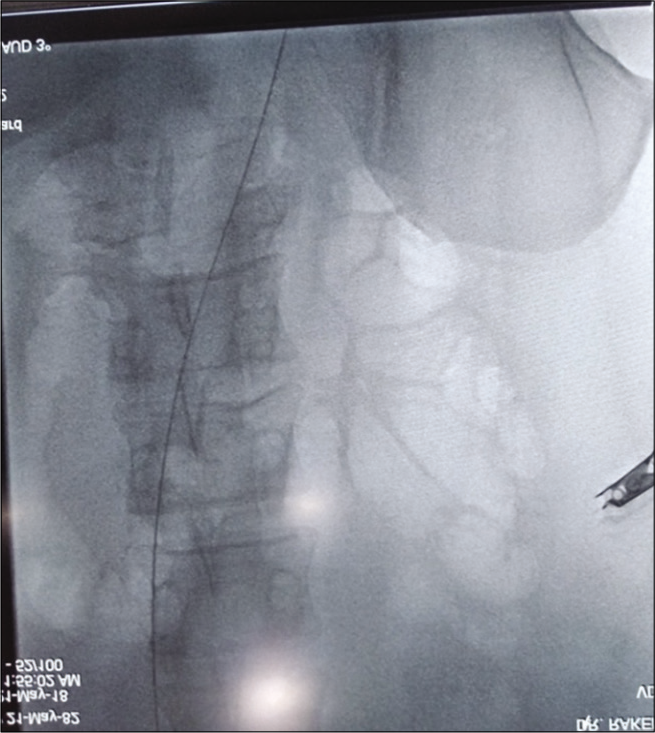
- The guidewire migrated into thorax.
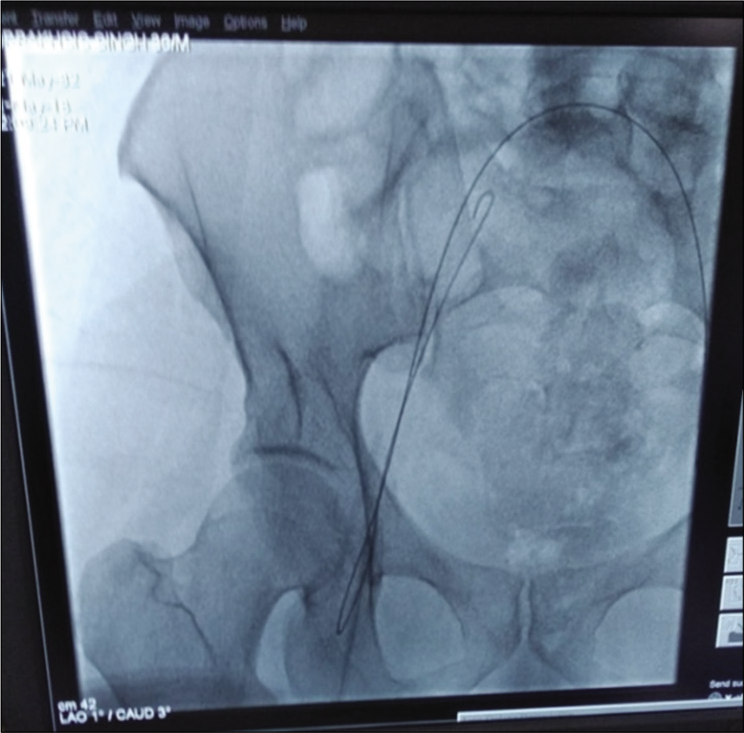
- The guidewire being removed under image guidance by gooseneck clamp.
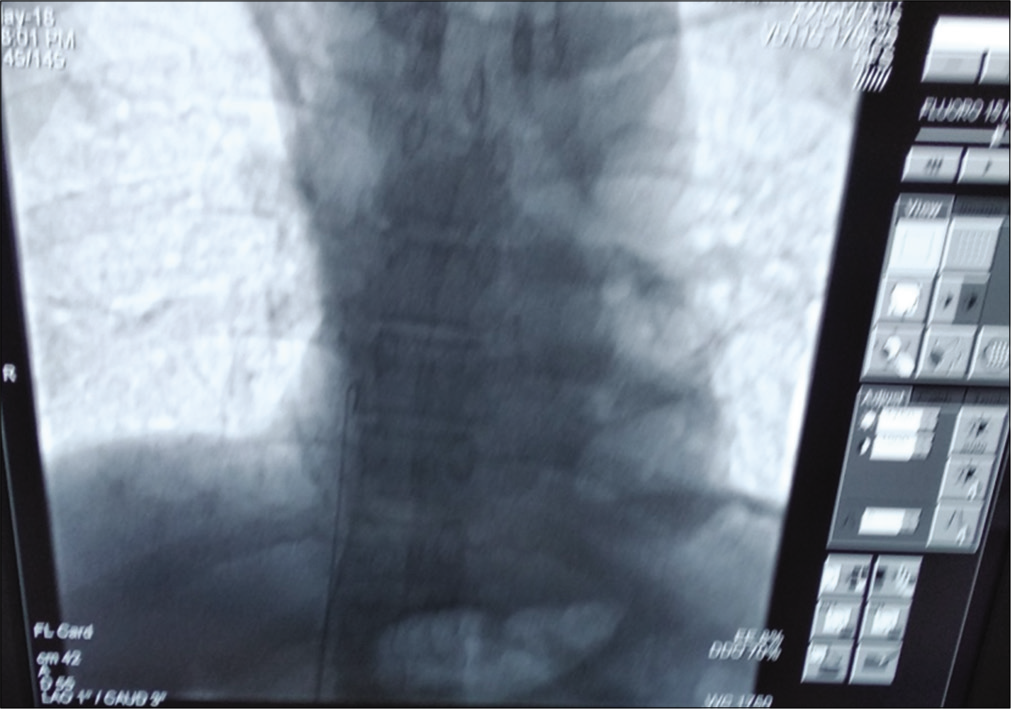
- The gooseneck clamp getting out the guidewire.
DISCUSSION
The guidewire should be held from the tip firmly with full attention during the procedure to prevent passage into or out of the vein. This rule should be followed strictly so that guidewire cannot get lost. In our case, the guidewire slipped unintentionally from consultant’s hand during cannulation in restless major burn patient who was not sedated in view of fear of losing airway and non-availability of patent intravascular access. The predisposing factors for an intravascular loss of the guidewire include inattention (almost all the cases), inexperienced operator (Seldinger’s technique), overtired staff and inadequate supervision of trainees.[1] The signs of guidewire loss include: Missing guidewire (as seen in our case)/visible on radiograph/poor venous backflow from the distal lumen/resistance to injection through the distal lumen.
Consequences of guidewire loss can include embolism from fragments of catheters or guidewires which can be fatal in up to 20% cases.[1] In contrast to such emboli, the loss of a complete guidewire usually does not cause symptoms. In general, the lost guidewire is found by chance on a radiograph.[5] There is insufficient data on the complications of lost guidewires although arrhythmias, vascular damage, thrombosis and embolism can occur with such foreign body. Ideally, faster insertion and removal of guidewire should be attempted. Interventional radiology is the method of choice to deal with lost catheter and by this entire guidewire should be removed urgently to avoid further manifestations.[1] During the removal, the patient is heparinized and the guidewire is caught by a gooseneck snare passed through the femoral vein using radiographic control as was done in our case.[6] Alternately the endovascular forceps or a Dornier basket could be used, though it increases the risk of endovascular trauma. It is necessary to remove the foreign body along the vascular sheath and it is possible when the sheath is twice the size of lost catheter/guidewire.[1] Surgical exploration is next modality for extraction of lost guidewire when heparinization of patient is contraindicated.
Serious complications can occur during each step of the central venous cannulation that needs to be understood by the operator and focused continuous attention is vital during procedure. Precautions should be taken with the Seldinger’s technique. The guidewire is delicate and fragile instrument and we need to inspect it for defects before insertion. When resistance to insertion is encountered, remove and inspect the wire for damage, reposition the introducer so that no resistance to its passage is felt. The central venous catheter placement in patients on thrombolytics, anticoagulants or who had repeated catheterizations of a particular vessel should be done cautiously. Using a J-tip style guidewire is a much safer practice.[4] We need to reinspect the guidewire if re-placement is necessary during multiple manipulations. During passage of catheter, the proximal end of guidewire should be held gently but firmly, before its advancement. Make sure the catheter and guidewire are not pushed together into the vein. The wire should not be advanced in the vein more than 18–20 cm in an adult patient.[7] At the end of procedure, the complete removal of guidewire should be recorded, both physically and radiologically. Ideally, hold the proximal end of the wire at all times until its removal from the vessel.
CONCLUSION
The central venous cannulation is a procedure requiring high expertise and meticulous attention. All trainees must be aware of all possible adverse outcomes of central line cannulation. Use of femoral approach is not a “choice” because, a slim but definite possibility of the catheter getting “sucked in” along with the venous flow as well as the negative intrathoracic pressure. Extreme patience and high attention are required of performing intensivist, as merely loss of concentration during any step can lead to complication as happened in our case. Holding of the guidewire during CVP cannulation is a crucial step and precautions need to be taken so as to avoid its slippage.
Acknowledgments
The authors want to acknowledge and feel indebted for the precise, timely and skillful help/intervention by Dr. Rakendra Singh (DM Cardiology), The Consultant Cardiologist, Department of Cardiology, in removing the lost guidewire.
Authors’ Contributions
The Dr. Goyal is the main author, did the major construction of the manuscript. Dr. Panditrao did the editing, refinement and final drafting of the manuscript. Dr. Garg was instrumental in most of the review of literature and compilation of the references, figures and other related work.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
- International evidence-based recommendations on ultrasound-guided vascular access. Intensive Care Med. 2012;38:1105-17.
- [CrossRef] [PubMed] [Google Scholar]
- A potentially hazardous complication during central venous catheterization: Lost guidewire retained in the patient. J Clin Anesth. 2012;24:221-6.
- [CrossRef] [PubMed] [Google Scholar]
- Guidewire-related complications during central venous catheter placement: A case report and review of the literature. Case Rep Crit Care. 2011;2011:287261.
- [CrossRef] [PubMed] [Google Scholar]
- The human error: Delayed diagnosis of intravascular loss of guidewires for central venous catheterization. J Clin Anesth. 2005;17:562-4.
- [CrossRef] [PubMed] [Google Scholar]
- Lost guide wire during central venous cannulation and its surgical retrieval. Indian J Surg. 2006;68:33-4.
- [Google Scholar]
- How much guidewire is too much? Direct measurement of the distance from subclavian and internal jugular vein access sites to the superior vena cava-atrial junction during central venous catheter placement. Crit Care Med. 2000;28:138-42.
- [CrossRef] [PubMed] [Google Scholar]




