

Translate this page into:
Normal human left ventricular mass, volume, and gender relationship by coronary computerized tomography angiography


*Corresponding author: Cetin Celenk, Department of Radiology, Ondokuz Mayis University, Istanbul, Turkey. ccelenk@hotmail.com
-
Received: ,
Accepted: ,
How to cite this article: Celenk V, Celenk C, Ozates M. Normal human left ventricular mass, volume, and gender relationship by coronary computerized tomography angiography. Adesh Univ J Med Sci Res 2023;5:69-73. doi: 10.25259/AUJMSR_19_2023
Abstract
Objectives:
There is a need to know the indexed heart values of people in each geographic region. The objective of this study is to establish normal reference values for the left ventricle.
Material and Methods:
Of the 450 caucasian adult patients who underwent coronary computed tomography angiography (CCTA) from June 2021 to March 2023, 310 meeting the appropriate criteria were selected for our retrospective study. The indication for CCTA triggered by a 384-detector retrospective electrocardiogram was screening for coronary artery disease (CAD) in people over 40 years of age. Patients with known CAD, heart failure, congenital heart disease, heart transplant, known allergies to X-ray contrast, or prior cardiac surgery were excluded from the study. We determined normal reference ranges for end-diastolic myocardial mass (EDMM), end-diastolic volume (EDV), and cursor volume (CV) using indexed body surface area (BSA).
Results:
BSA indexed values are EDMM = 76 and 60g/m2, EDV = 65 and 61 mL/m2, CV = 46 and 42 mL/m2, heat index = 178 and 160 cm, weight = 89 and 81 kg, age = 55 and 57 years, and heart rate = 60 and 63 for men and women, respectively; 95% confidence interval.
Conclusion:
All parameters were different between males and females. In this cross-sectional general population study, men had significantly more indexed left ventricular mass than women (P < 0.01), with no significant differences between men and women in all other parameters (P > 0.05). These values indicate ethnic diversity.
Keywords
Coronary angiography
Computerized tomography
Myocardium
Normative values
Left ventricle
Volume

INTRODUCTION
The adoption of electrocardiogram (ECG)-triggered acquisition of coronary computed tomography angiography (CCTA) has resulted in the ability to measure ventricular values. Left ventricular (LV) mass and volume parameters can be obtained from a large number of normal subjects using transthoracic echocardiography (TTE), magnetic resonance imaging (MRI), and computerized tomography (CT).[1-11] Perspicuously, these factors may be important in defining normal values. CCTA has been developed as an important clinical method for patients suspected to have cardiac disease, with a substantial expansion in worldwide use in recent years.[4-6,11] Normal values of LV mass, volume, and cursor index parameters in asymptomatic cases are a prerequisite for the diagnosis of individuals at risk for heart disease.[12,13]
CT images allow for accurate assessment of LV myocardial mass (LVMM) and LV end-diastolic volume (EDV) parameters. These values are similar to MRI and TTE results. Therefore, it is possible to obtain valuable information in addition to the well-established coronary assessment obtained from these images.[4-6,11]
The aims of this study were to (1) validate the accuracy of CT for LV mass and volume measurements, (2) establish the normal range of LV mass and volume index in healthy subjects, and (3) investigate the effects of age and gender on LV mass and volume index.
MATERIAL AND METHODS
Study population
This retrospective, observational cohort study received an institutional review board (IRB-2022/68-39) approval. All participants gave informed consent for the CCTA protocol and study. We evaluated 310 participants with no previous history of cardiovascular disease retrospectively. The patients were 193 men (mean age 55 years, range 40–77 years) and 117 women (mean age 57 years, range 42–76 years). Table 1 describes the participants characteristics (ventricular parameters normalized to body surface area [BSA], weight, and height).
| Male (n=193) | Female (n=117) | All (n=310) | ||||
|---|---|---|---|---|---|---|
| Mean±Std.Dev. | %95 CI | Mean±Std.Dev. | %95 CI | Mean±Std.Dev. | %95 CI | |
| Lower; Upper | Lower; Upper | Lower; Upper | ||||
| EF % | 71,45±5,30 | 69,43; 73,47 | 73,17±8,28 | 69,67; 76,66 | 69,57±8,60 | 61,62; 77,52 |
| EDMM (g/m2) | 76,22±18,11 | 69,33; 83,11 | 60,24±8,27 | 56,75; 63,73 | 68,10±8,78 | 59,98; 76,22 |
| EDV mL/m2 | 65,19±12,62 | 60,38; 69,99 | 61,43±13,70 | 55,65; 67,22 | 61,19±21,47 | 41,33; 81,04 |
| CV mL/m2 | 46,37±12,48 | 41,63; 51,12 | 42,05±13,33 | 36,42; 47,68 | 49,50±15,21 | 35,43; 63,57 |
| Height cm | 177,96±5,47 | 175,84; 180,09 | 160,75±7,05 | 157,77; 163,73 | 170,57±13,07 | 158,48; 182,66 |
| Weight kg | 89,25±9,70 | 85,49; 93,01 | 80,92±16,40 | 73,99; 87,84 | 87,43±15,10 | 73,47; 101,39 |
| HR/min. | 60,29±5,44 | 55,26; 65,32 | 63,14±3,24 | 60,15; 66,14 | 64,14±3,34 | 61,06; 67,23 |
| BSA/m2 | 2,11±0,12 | 2,03; 2,18 | 1,98±0,18 | 1,86; 2,11 | 2,03±0,17 | 1,88; 2,19 |
EDMM: Enddiastolic myocardial mass, EDV: Enddiastolic volume, CV: Cursor volume, HR: Heart rate, BSA: Body surface area, CI: Confidence interval, EF: Ejection fraction
Of the 450 participants, 130 (54%) were excluded due to the presence of 1 or more cardiovascular risk factors; incomplete demographic or blood sample data; missing spirometry, ECG, contrast scan, or diastole scan; inadequate image quality or software segmentation for chamber assessment; calcium scoring; or coronary artery evaluation.
We report results for participants who underwent CCTA, excluding participants with any of the following characteristics: (1) coronary artery disease (CAD); (2) cardiovascular disease (self-reported previous myocardial infarction, coronary bypass, percutaneous coronary intervention, or stroke); (3) hypertension; (4) hypercholesterolemia; (5) taking cardiovascular prescription medication, including diuretics, statins, or aspirin; (6) overweight (defined as BMI ≥25); (7) diabetes mellitus (self-reported or blood glucose of 0.8 mmol/L); (8) chronic obstructive pulmonary disease; (9) coronary artery anomaly; and (10) ECG abnormalities.[1,6,10,14]
CCTA procedure
We examined the Siemens Edge device with 384 sections with a section thickness of 0.5 mm, using the ECG gating/retrospective method. We evaluated the images with the Siemens workstation (Syngo Via) program package [Figure 1]. For each angiographic projection, the workstation program automatically detected the lumen border. We chose the tube voltage and current based on the participants’ BMI, ranging between 20 and 120 kV and 20 and 600 mAs, respectively. A cardio-selective beta-blocker (metoprolol 25–150 mg) was administered orally 1 h before scanning in participants with a heart rate of >70 beats per minute and no contraindications. An intravenous line (18 gauge) was inserted in the antecubital vein. The amount was automatically determined by the device according to BSA Visipaque (320 mg/mL) and infused with a flow rate of 5 mL/s in three phases (approximately 70–85 mL). The first phase used approximately 65 mL of contrast, the second phase used 15 mL of contrast and 6 mL of saline, and the third phase used 50 mL of saline. Image acquisition triggering was set at an aortic attenuation density of 180 Hounsfield units. In participants with known allergies to X-ray contrast, no contrast was given. We conducted ECG gating with dose modulation and reconstructed images at the R-R interval. The program determined the best end-diastole phases according to the contrasting volumes. Our device has an automated least motion-free phase algorithm to optimize images for coronary artery evaluation. In general, 70–75% had the best end-diastole.
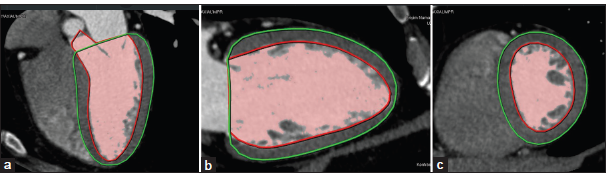
- (a) Sagittal oblique, (b) coronal oblique, (c) axial slices shows typical examples of the auto-contouring of the endocardial (red) and epicardial (green) contouring using Syngo through a middiastolic prospectively electrocardiogram-triggered coronary computed tomography angiography.
Image analysis and determination of ventricular parameters
We transferred the images to an independent workstation (Syngo Via) for analysis. The program is automatically processed by selecting the best end-diastolic images. The LV endocardial and epicardial borders were semi automatically determined at end-diastole using CT software. By placing a seed point in the colored area, the edges of the colored area are semi automatically detected and outlined [Figure 1a-c]. The user may then switch back to a pure grayscale image and edit the borders. Myocardial mass is determined by multiplying the myocardial tissue in g/cm3.
RESULTS
First, we conducted the Shapiro–Wilk test to establish normal distribution, and the features were not compatible with normal distribution in end-diastolic myocardial mass (EDMM), EDV, or CV (P <.05). We compared these features according to gender using the Mann–Whitney U test, and we compared other features compatible with the normal distribution with the independent group t-test [Table 2]. We provide the results below.
| t-test for equality of means | Mann–Whitney P-value | |||
|---|---|---|---|---|
| t | df | Sig. (2-tailed) | Sig. (2-tailed) | |
| Height cm | 9.906 | 50,000 | 0.000 | |
| Weight kg | 2.183 | 36,093 | 0.036 | |
| EF% | −0.879 | 37,706 | 0.385 | 0.149 |
| EDMM (g/m2) | 3.988 | 51,000 | 0.000 | 0.000 |
| EDV mL/m2 | 1.036 | 51,000 | 0.305 | |
| CV mL/m2 | 1.217 | 51,000 | 0.229 | |
| HR | −1.195 | 12,000 | 0.255 | |
| BSA/m2 | 1.903 | 20,000 | 0.072 | |
EDMM: Left ventricular enddiastolic myocardial mass, EDV: Enddiastolic volume, CV: Left ventricular cursor volume, HR: Heart rate; BSA: Body surface area. There is a significant difference between the mean EDMM and height of males and females (P<0.001), There is a significant difference between the mean weights of men and women (P=0.036), There is no significant difference in the other characteristics ofmen and women (P>0.05), EF: Ejection fraction, t: T value, df: Degree of freedom, Sig: Significance
There is a very significant difference between the average heights of men and women (P < 0.001)
There is a significant difference between the mean weights of men and women (P = 0.036)
There is a very significant difference between the median EDMMs of men and women (P < 0.001)
There is no significant difference between the other characteristics of men and women (P > 0.05).
DISCUSSION
In this cross-sectional study, we determined normal values for EDMM, EDV, and CV from CCTA images of healthy individuals in a certain age group. It has been found that LVMM is intimately related to lean body mass.[14]
In our study, gender differences were not apparent in all ventricular parameters measured for the LV end-diastolic (LVED) volume ratio.
Power calculations indicated that the sample sizes used in this study were sufficient for detecting these gender differences with a power greater than 90%. All mass parameters were smaller in females than in males; these findings are consistent with those of other researchers in CT and MRI studies.[1-7,9-11]
We found distinct differences in LV mass related to gender, demonstrating the need for gender-specific normal CCTA values. We provide such values for future diagnostic purposes in patients suspected of cardiac disease undergoing CCTA. One of the most important tasks in patient examination, including cardiac imaging, is to distinguish normal findings from those indicative of disease. Normal ranges for a given parameter encompassing 95% of the population constitute the mainstay of this practice. Chamber volumes and LVMM have high predictive value in various patient groups in terms of prognosis, including patients with cardiovascular disease, which needs to be documented in long-term follow-up studies. CCTA is widely accepted for the examination of coronary arteries.
However, the lack of normal values for LV mass and cardiac chamber dimensions assessed with this type of imaging limits the full-scale clinical utility of CCTA. Our values for LV mass and cardiac chamber dimensions in end-diastole are generally consistent with previous studies [Table 2].[1-11] In previous studies using the BSA index, women’s LVMM and volume values have generally been lower than men’s.[1-11] In our study, LVMM values were significantly lower in women, and LV volume values were slightly low [Table 1]. Our results demonstrate that men have significantly greater indexed LVMM than women, in concordance with earlier MRI and CT studies.[1-7,9-11]
Mizukoshi et al. found a difference in EDV between men and women in a TTE study in Japanese and American populations but found no difference in EDMM.[8]
Previous MRI and CT results show that men have significantly higher absolute and indexed LVM and LV diastolic volume (LVDV).[1-7,9-11] However, we only found LVMM-indexed values higher in males than females. We found no significant difference between men and women in LVDV values.
Earlier studies showed that BSA, gender, systolic blood pressure, and hard physical activity are factors associated with LVMM.[6,13,15]
Women’s lower EDMM values are probably due to physical activity. However, further studies are needed to confirm this hypothesis.
This study’s results indicate that when determining whether an individual’s ventricular parameters fall into normal ranges, parameters related to function and relative LV hypertrophy are relatively gender-independent (LVED volume, ejection fraction, and cardiac output), except LVMM.
The study is limited by the sample size; we could have made more robust statistical calculations with subgroups of larger sample sizes. Our study included only a certain age group of caucasian adults; therefore, our data may not be relevant for other populations and other age groups.
CONCLUSION
Using low-dose, contemporary CCTA, we established normal values for the assessment of LV mass and volume. Significant differences in these measurements are particularly related to gender and age, as well as other factors. These findings demonstrate the need for physiologic activity-, age-, and gender-specific CCTA normal values and provide such values for future diagnostic purposes in patients suspected of having cardiac disease. This study ensures a range of normal ventricular parameters for females and males that can be used to identify abnormal volume for mass in the left ventricle. Our study has shown that morphologic parameters remain gender dependent. These results can serve as a reference for studying diseases that affect the left ventricle.
Ethical approval
The research/study is approved by the Institutional Review Board at Biruni University, number (IRB-2022/68-39).
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent.
Conflicts of interest
There are no conflicts of interest.
Use of artificial intelligence (AI)-assisted technology for manuscript preparation
The authors confirm that there was no use of artificial intelligence (AI)-assisted technology for assisting in the writing or editing of the manuscript and no images were manipulated using AI.
Financial support and sponsorship
Nil.
References
- Normal human right and left ventricular mass, systolic function, and gender differences by cine magnetic resonance imaging. J Cardiovasc Magn Reson. 1999;1:7-21.
- [CrossRef] [PubMed] [Google Scholar]
- Estimation of human myocardial mass with MR imaging. Radiology. 1988;169:495-8.
- [CrossRef] [PubMed] [Google Scholar]
- Evaluation of left ventricular volumes measured by magnetic resonance imaging. Eur Heart J. 1986;7:1016-21.
- [CrossRef] [PubMed] [Google Scholar]
- Normal values of left ventricular mass and cardiac chamber volumes assessed by 320-detector computed tomography angiography in the Copenhagen General Population Study. Eur Heart J Cardiovasc Imaging. 2016;17:1009-17.
- [CrossRef] [PubMed] [Google Scholar]
- Cardiac CT assessment of left ventricular mass in mid-diastasis and its prognostic value. Eur Heart J Cardiovasc Imaging. 2017;18:95-102.
- [CrossRef] [PubMed] [Google Scholar]
- Mid-diastolic left ventricular volume and mass: Normal values for coronary computed tomography angiography. J Cardiovasc Comput Tomogr. 2017;11:135-40.
- [CrossRef] [PubMed] [Google Scholar]
- Sex-and age-specific normal values of left ventricular functional and myocardial mass parameters using threshold-based trabeculae quantification. PLoS One. 2021;16:e0258362.
- [CrossRef] [PubMed] [Google Scholar]
- Normal values of left ventricular mass index assessed by transthoracic three-dimensional echocardiography. J Am Soc Echocardiogr. 2016;29:51-61.
- [CrossRef] [PubMed] [Google Scholar]
- Impact of age, sex, and indexation method on MR left ventricular reference values in the Framingham Heart Study offspring cohort. J Magn Reson Imaging. 2015;41:1038-45.
- [CrossRef] [PubMed] [Google Scholar]
- Normalized left ventricular systolic and diastolic function by steady state free precession cardiovascular magnetic resonance. J Cardiovasc Magn Reson. 2006;8:417-26.
- [CrossRef] [PubMed] [Google Scholar]
- Reference absolute and indexed values for left and right ventricular volume, function and mass from cardiac computed tomography. J Med Imaging Radiat Oncol. 2014;58:547-58.
- [CrossRef] [PubMed] [Google Scholar]
- Myocardial bridging, a frequent component of the hypertrophic cardiomyopathy phenotype, lacks systematic association with sudden cardiac death. Eur Heart J. 2009;30:1627-34.
- [CrossRef] [PubMed] [Google Scholar]
- Clinical course and management of hypertrophic cardiomyopathy. N Engl J Med. 2018;379:655-68.
- [CrossRef] [PubMed] [Google Scholar]
- Effect of lean body mass, fat mass, blood pressure, and sexual maturation on left ventricular mass in children and adolescents. Statistical, biological, and clinical significance. Circulation. 1995;92:3249-54.
- [CrossRef] [PubMed] [Google Scholar]
- European Guidelines on cardiovascular disease prevention in clinical practice (version 2012): The Fifth Joint Task Force of the European Society of Cardiology and Other Societies on Cardiovascular Disease Prevention in Clinical Practice (constituted by representatives of nine societies and by invited experts) Eur Heart J. 2012;33:1635-701.
- [CrossRef] [PubMed] [Google Scholar]




