

Translate this page into:
“Meckel’s Diverticulum” – A diagnostic bizarre of abdominal pain in adults

*Corresponding author: Dr. Vipin Kumar Bakshi, Departments of Radio- diagnosis, Adesh Institute of Medical Sciences and Research, Bathinda, Punjab, India. drvipinbakshi@yahoo.com
-
Received: ,
Accepted: ,
How to cite this article: Bakshi VK, Kaur M, Bhatti G. “Meckel’s Diverticulum” – A diagnostic bizarre of abdominal pain in adults. Adesh Univ J Med Sci Res 2020;2(1): 58-60.
Abstract
A 30-year-old male presented to the emergency room with complaints of periumbilical abdominal pain and vomiting. A contrast-enhanced computed tomography scan of the abdomen revealed subacute intestinal obstruction with dilated small bowel loops and associated bowel wall thickening of mid and distal ileal bowel loops. There was a fairly large small bowel diverticulum arising from the antimesenteric border of distal ileum. Findings were suggestive of small bowel diverticulitis or possibly focal enteritis. The patient was then immediately taken to the operating room for emergency laparotomy and was intra-operatively found to have a thickened Meckel’s diverticulitis with adjacent small bowel obstruction. Meckel’s diverticulectomy was performed in continuity with the adjacent inflamed small bowel. The patient had a stable post-operative course without any complications and was discharged within a week.
Keywords
Meckel’s diverticulum
Congenital diverticulum
Abdominal pain
Contrast-enhanced computed tomography abdomen subacute intestinal obstruction

INTRODUCTION
Meckel’s diverticulum (MD), a congenital distal ileal diverticulum, is the most common congenital anomaly of the gastrointestinal tract; it is considered a remnant of the omphalomesenteric vitelline duct, which connects the yolk sac to the midgut through the umbilical cord. This duct is typically obliterated by the 5–8th week of gestation. Failure of closure results in the formation of a true diverticulum of the small intestine.[1] Meckel’s diverticula are uncommon and often clinically silent, particularly in adults. Asymptomatic MD may be discovered during abdominal exploration for the evaluation of unrelated pathology. At times, Meckel’s diverticula are found incidentally on diagnostic imaging. When symptomatic, MD may present with abdominal pain or symptoms of gastrointestinal bleeding or bowel obstruction.[1]
MD is a true diverticulum (i.e., all layers of the gastrointestinal tract are present in its wall) and arises from the antimesenteric border of the small intestine. It can be as long as 5 cm with diameters up to 2 cm. Most (75%) Meckel’s diverticula are found within 60 cm (range 40–100 cm) of the ileocecal valve.[2] It can be seen in the midline, or on either side of the midline. However, midline and right iliac fossa location are the commonest. Its level on computed tomography (CT) can be either superior or inferior to the terminal ileum.[3]
Here, we report a case of Meckel’s diverticulitis in a 30-year-old male who presented with abdominal pain.
CASE REPORT
A 30-year-old male presented to the emergency room of our hospital with complaints of periumbilical abdominal pain that started while he was having lunch the same day. The pain was severe in intensity, not radiating, sharp, with no aggravating or relieving factors. The abdominal pain was associated with nausea and multiple episodes of non-bloody, bilious vomiting.
On physical examination, the patient was afebrile (98.6°F) and hemodynamically stable with a pulse rate of 94 beats/min, respiratory rate of 19 breaths/minute, blood pressure of 138/98 mm Hg, and oxygen saturation of 94% on room air. The abdomen was soft with periumbilical tenderness and audible bowel sounds.
Laboratory testing revealed leukocytosis with neutrophilia and a normal hemoglobin count. Contrast-enhanced CT scan of the abdomen revealed subacute intestinal obstruction with significant dilatation of small bowel loops up to mid ileum with zone of transition between dilated and non-dilated loop in right lower abdomen with twisting/adhesion of ileal bowel loops in the distal ileum [Figure 1]. There was a fairly large small bowel diverticulum associated with this segment [Figure 2]. Findings were suggestive of small bowel diverticulitis or possibly focal enteritis. The patient was then immediately taken to the operating room for emergency laparotomy and was intra- operatively found to have a thickened Meckel’s diverticulitis with adjacent small bowel obstruction [Figure 3]. Meckel’s diverticulectomy was performed in continuity with the adjacent inflamed small bowel. The pathology report later revealed an MD with suppurative diverticulitis, abscess, and acute mucosal inflammation.
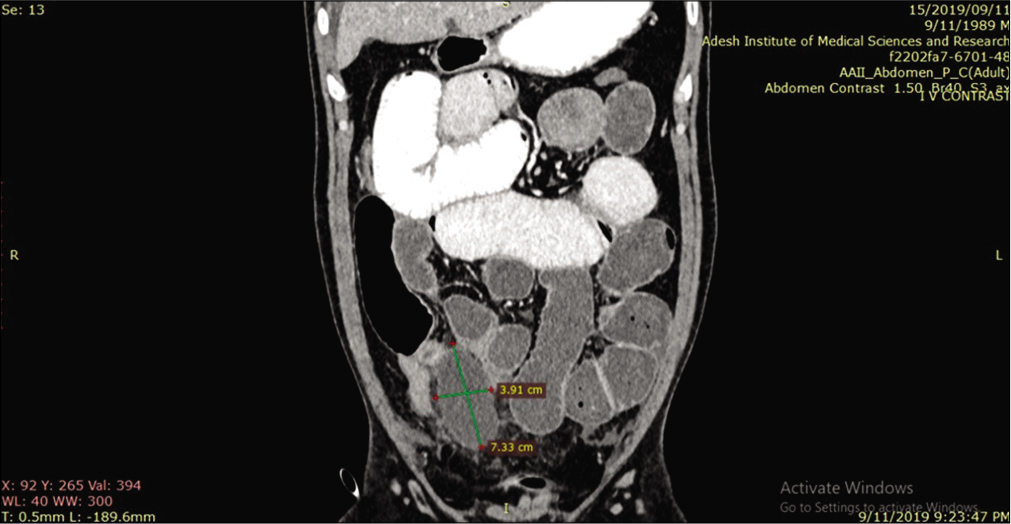
- Contrast-enhanced computed tomography abdomen – coronal reformation showing Meckel’s diverticulum (measured outpouching) with dilated small bowel loops.
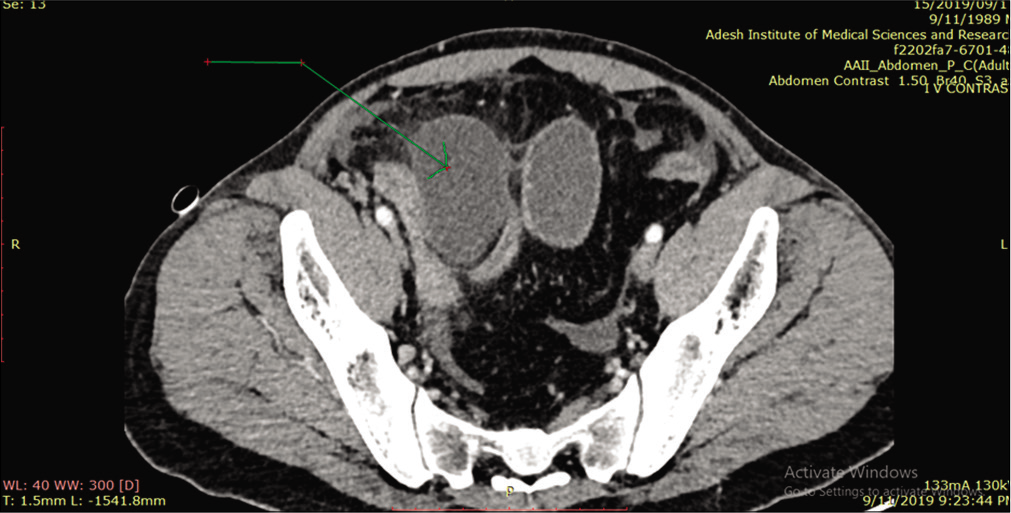
- Contrast-enhanced computed tomography abdomen – axial reformation showing Meckel’s diverticulum (arrow) with imperceptible bowel wall.

- Intraoperative picture showing gangrenous Meckel’s diverticulum.
The patient had a stable post-operative course without any complications and was discharged within a week.
DISCUSSION
Although this diverticulum was first identified by German surgeon Wilhelm Fabricius Hildanus in 1598, it was German pathologist Johan Friedrich Meckel who described it in detail and discovered its embryologic origin in 1809.[4,5]
Conventionally, salient features of MD are described in a “rule of 2s” as a useful memory aid, although the exact ratio may vary:[6] They are present in 2% of the population, they are 2 ft (60 cm) proximal to the ileocecal valve, they are 2 in (5 cm) long, approximately two-thirds of cases have ectopic mucosa, there are two types of mucosa in bleeding diverticulum (native intestinal and ectopic gastric), there are two types of ectopic mucosa (gastric and pancreatic), 2% of patients develop complications or symptoms, they usually present before the age of 2 years, and they are two times as likely to be symptomatic in male patients as in female patients.
MD rarely causes symptoms in adults and typically is overlooked in imaging studies when uncomplicated. However, complications may occur. Several complications are associated with MD, including intestinal obstruction, hemorrhage, diverticulitis, perforation, and formation of neoplasm and enterolith. Conventionally, it is described that bleeding is the most common complication in children. In adults, obstruction and diverticulitis are more common. Since cross-sectional imaging is commonly used in these clinical situations, the radiologist should be familiar with the normal imaging appearance of MD and its potential complications. On encountering a blind- ending structure in the right lower quadrant, the radiologist should confirm the presence of a separate appendix and confirm the connection of the structure with the ileum rather than the cecum before making the diagnosis of MD or diverticulitis. The pre-operative diagnosis of MD in small-bowel obstruction is extremely difficult, but it should be offered as a differential diagnosis consideration in young adults with bowel obstruction with no obvious cause and no surgical history, especially if the zone of transition is in the expected location of MD.[7,8]
In patients with symptomatic MD, the challenge presents itself in early diagnosis and prompt surgical treatment. As it is a rare condition, a high index of suspicion is necessary as clinical presentation is variable, differential diagnosis is not straightforward, and imaging techniques may not be useful at times. To overcome these difficulties, a CT scan with oral and intravenous contrast (if possible) is recommended. In the case of our patient, we were able to make the diagnosis preoperatively, perform the surgery promptly, and were able to avoid complications of delayed surgical intervention.
Authors’ contributions
All authors have made contributions to the article and have reviewed it before submission.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent forms.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
- Meckel's diverticulum: A systematic review. J R Soc Med. 2006;99:501-5.
- [CrossRef] [PubMed] [Google Scholar]
- Imaging manifestations of Meckel's diverticulum. AJR Am J Roentgenol. 2007;189:81-8.
- [CrossRef] [PubMed] [Google Scholar]
- Johann Friedrich Meckel the younger: Meckel's diverticulum. Gastrointest Endosc. 2001;54:19A-20A.
- [Google Scholar]
- Reminiscing on remnants: Imaging of Meckel diverticulum and its complications in adults. AJR Am J Roentgenol. 2017;209:W287-96.
- [CrossRef] [PubMed] [Google Scholar]
- A rare cause of abdominal pain in adults: Meckel's diverticulitis. Case Rep Gastroenterol. 2018;12:709-14.
- [CrossRef] [PubMed] [Google Scholar]




