

Translate this page into:
A comparison of the new parameter, “MKG angle” with ANB, Wits’ appraisal, Yen, Pi, and W angles

*Corresponding author: Alisha Babbar, Department of Orthodontics and Dentofacial Orthopedics, Adesh Dental College, Gidderbaha, Punjab, India. dralishachuchra@gmail.com
-
Received: ,
Accepted: ,
How to cite this article: Babbar A, Bansal N, Sunda S, Babbar A. A comparison of the new parameter, “MKG angle” with ANB, Wits’ appraisal, Yen, Pi, and W angles. Adesh Univ J Med Sci Res 2023;5:74-7. doi: 10.25259/AUJMSR_20_2023
Abstract
Objectives:
The objectives of the study are to compare and assess the precision of MKG angle with ANB, Wits’ appraisal, Yen, Pi, and W angles and reproducibility between them.
Material and Methods:
160 pre-treatment cephalograms of 80 skeletal class I and 80 skeletal class II patients were selected from the Department of Orthodontics and Dentofacial Orthopedics and were divided into Group 1 and Group 2. MKG angle, ANB angle, Wits’ appraisal, W, Yen, and Pi angles were measured, and MKG angle was compared with each of them for the evaluation of its precision.
Results:
The statistical analysis was done using SPSS software version 26.0. The mean, standard deviation, t-test, and Pearson correlation coefficient were calculated. Descriptive statistics were done to know the mean and standard deviation. The Pearson correlation coefficient was done to know the correlation between the MKG angle and other parameters in both the groups. A statistically significant difference was observed between MKG angle and all other parameters – ANB, Wits’ appraisal, YEN, W, Pi angles in general population.
Conclusion:
MKG angle can be used to assess the anteroposterior discrepancy but as an adjunct with other parameters.
Keywords
MKG angle
ANB
Wits’ appraisal
Yen
Pie
W angle

INTRODUCTION
The assessment of the anteroposterior skeletal jaw relationship is one of the most crucial diagnostic decisions for an orthodontist to take before treatment planning. For this reason, there were plenty of cephalometric analyses[1] in literature, but none of them is flawless. Hence, there is a need to embrace the perpetual pursuit for better methods of diagnosis. The ANB angle, which is considered the golden standard in assessing an anteroposterior jaw relationship, has its limitations, like the nasion being unstable with age, thus questioning the reliability of this angle. To overcome these problems, Jacobson introduced Wits’ appraisal, which is a linear measurement, but this is not dependable as it describes the changes in the occlusal plane but not the anteroposterior changes. For this reason, a measurement unconstrained of the cranial reference planes or dental occlusion would be favorable for an orthodontist in determining the apical base relationship. Addressing this requisite Yen (Yenepoya angle),[2] W[3] and Pi[4] angles were introduced, which also have their apparent advantages and limitations, such as the Yen angle relying on point S, and the true horizontal plane in Pi analysis passing through nasion, which again are the unstable landmarks.[5] Hence, a new parameter MKG angle[6] is proposed using the key ridge,[7] which remains constant in the cranial bones throughout the life to assess the anteroposterior jaw relationship.[8] Thus, the aim of the present study was to compare the MKG angle with ANB, Wits’ appraisal, Yen, Pi, and W angles and to assess the precision and reproducibility between them.
MATERIAL AND METHODS
The present retrospective study was conducted on 160 pre-treatment cephalograms of 80 skeletal class I and 80 skeletal class II patients after sample size calculation by statistician from records of the Department of Orthodontics and Dentofacial Orthopedics Genesis Institute of Dental Sciences (GIDSR), Ferozepur. The ethical clearance was taken from the ethical committee GIDSR, Ferozepur, before the start of the study. Lateral cephalograms selected were based on certain inclusion and exclusion criteria. The lateral cephalograms included were Class I subjects with an ANB angle of 2°–4°, Wits’ appraisal 0–4 mm, Yen angle 117°–123°, W angle 51°–56°, Pi angle 2.9°+2.533°, and MKG angle 51°–59° and Class II subjects with an ANB angle of >4°, Wits’ appraisal >4 mm, Yen angle <117°, and W angle 59°. The patients included in the study had permanent dentition with no missing teeth and age group of 15–25 years. The patients who had undergone prior orthodontic treatment and had any cranial or facial malformations or cephalograms of poor quality were excluded from the study.
All cephalograms were traced using a sharp 0.5 mm pencil on acetate tracing paper using X-ray viewer. The sample was then divided into 2 groups - Group 1 skeletal class I and Group 2 skeletal class II patients. MKG angle, ANB angle, Wits’ appraisal, W, Yen, and Pi angles were then measured, and MKG angle was compared with each of them for the evaluation of its precision [Figure 1].
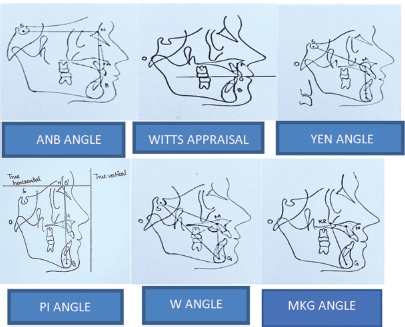
- Measured angles.
The statistical analysis was done using SPSS software version 26.0. The mean, standard deviation, t-test, and Pearson correlation coefficient were calculated. Descriptive statistics was done to determine the mean and standard deviation, and the Pearson correlation coefficient was done to determine the correlation between the MKG angle and other parameters in both groups.
RESULTS
The present study was carried out on 160 pre-treatment cephalograms to know the correlation between MKG angle and other parameters in both groups.
The Pearson correlation coefficient was done, and a significant difference was observed between MKG and all other parameters – ANB, Wits’ appraisal, YEN, W, Pi angles in the general population [Table 1]. A significant correlation between the MKG angle and ANB angle (P = 0.581), Wits’ appraisal (P = 0.504), and Pi angle (P = 0.617) were observed, and there is a significant negative correlation between MKG angle and YEN angle (P = −0.629) and W angle (P = −0.604).
| Correlations | |||||
|---|---|---|---|---|---|
| ANB (degrees) | Wits’ appraisal (mm) | Yen (degrees) | W (degrees) | Pi (degrees) | |
| MKG (degrees) | |||||
| Pearson Correlation | 0.581** | 0.504** | −0.629** | −0.604** | 0.617** |
| Sig. (2-tailed) | 0.000 | 0.000 | 0.000 | 0.000 | 0.000 |
| N | 160 | 160 | 160 | 160 | 160 |
Group 1 shows no statistically significant correlation between the MKG angle and ANB, Wits’, Pi angles, but a statistically significant negative correlation was observed between the MKG angle and Yen angle (P = −0.416) and W angle (P = −0.295). There is a statistically significant difference observed between MKG angle and Yen, W, Pi angles but no significant difference between MKG angle and ANB, Witsi appraisal [Table 2].
| Skeletal class I | ANB (degrees) | Wits’ appraisal (mm) | Yen (degrees) | W (degrees) | Pi (degree s) |
|---|---|---|---|---|---|
| MKG (degrees) | |||||
| Pearson Correlation | 0.207 | −0.037 | −0.416** | −0.295** | 0.212 |
| Sig. (2-tailed) | 0.066 | 0.744 | 0.000 | 0.008 | 0.059 |
| N | 80 | 80 | 80 | 80 | 80 |
Group 2 shows a statistically significant correlation between the MKG angle and the Pi angle (P = 0.348) but the other parameters ANB, Wits, YEN, W angles were not significantly correlated with MKG angle and there is statistically significant difference between the MKG angle and Pi angle (P = 0.002) but no significant difference between the MKG angle and ANB, Wits, Yen, W angles [Table 3].
| Correlations | |||||
|---|---|---|---|---|---|
| Skeletal class II | ANB (degrees) | Wits’ appraisal (mm) | Yen (degrees) | W (degrees) | Pi (degrees) |
| MKG (Degrees) | |||||
| Pearson Correlation | 0.179 | 0.129 | −0.147 | −0.123 | 0.348** |
| Sig. (2-tailed) | 0.111 | 0.252 | 0.194 | 0.278 | 0.002 |
| N | 80 | 80 | 80 | 80 | 80 |
DISCUSSION
The main aim of the orthodontic treatment is to correct the sagittal discrepancies. Various parameters had been used to evaluate the sagittal discrepancies which include ANB angle, WITS appraisal and BETA angle which have some disadvantages. Later YEN, W, HBN and TAU are introduced. This study mainly discuss about the accuracy of newer parameter MKG angle in evaluating the sagittal discrepancies in comparison with ANB,beta, yen and pie angle. The comparison in our study was done in order to evaluate the reliability of MKG angle in evaluating the sagittal discrepancy.
In Present study we evaluated the accuracy of MKG angle in determining the sagittal discrepancies. MKG angle is introduced by Dr Achinth chachada. The main purpose of introducing the MKG angle in orthodontics is an accurate AP measurement of jaw relationships which is critically important in orthodontic treatment planning. ANB is still widely used, but it is affected by various factors and can often be misleading. To overcome these difficulties MKG angle was developed.
The MKG angle does not depend on cranial landmarks or the functional occlusion plane and point A and point B. It has three landmarks such as the key ridge, M midpoint of the premaxilla, and G center of the largest circle that is tangent to the internal inferior, anterior, and posterior surfaces of the mandibular symphysis which does not change with age.
The present study was carried on 160 pre treatment cephalogram of 80 skeletal class I and 80 skeletal class II and MKG angle, ANB angle, Beta angle, yen and pie angle was measured and MKG angle was compared with each of them for the evaluation of its precision.
The results of this study shows statistically significant difference between MKG angle and Yen, W, Pi angles but no significant difference between MKG angle and ANB, Witts’s appraisal.
In skeletal class I patients there is statistically significant correlation between the MKG angle and the Pi angle but the other parameters ANB, Witts, YEN, W angles were not significantly correlated with MKG angle.
In skeletal class II patients there is statistically significant difference between the MKG angle and Pi angle but no significant difference between the MKG angle and ANB, Witts, Yen, W angles.
Based on the results of this study it can be said that MKG angle can be used to assess sagittal jaw relationship with high reliability. But only one parameter should not be used to determine anteroposterior dysplasia as all other parameters correlate with each other.
Any clinician should be aware of as many cephalometric analysis as possible but should use them cautiously and appropriately. By relying on single parameter that was developed years ago without periodically reevaluating it , the diagnosis and treatment planning can be insufficient.
Further studies need to be done with more sample size and gender differences.
CONCLUSION
MKG angle can be used for assessing anteroposterior discrepancy but as an adjunct with other parameters.
Ethical approval
The research/study complied with the Helsinki Declaration of 1964.
Declaration of patient consent
Patient’s consent not required as patients identity is not disclosed or compromised.
Conflicts of interest
There are no conflicts of interest.
Use of artificial intelligence (AI)-assisted technology for manuscript preparation
The authors confirm that there was no use of artificial intelligence (AI)-assisted technology for assisting in the writing or editing of the manuscript and no images were manipulated using AI.
Financial support and sponsorship
Nil.
References
- An evaluation of centrographic analysis as compared with conventional cephalometric analysis. J Ind Orthod Soc. 2012;46:38-42.
- [CrossRef] [Google Scholar]
- A new approach of assessing sagittal dysplasia: The W angle. Eur J Orthod. 2013;35:66-70.
- [CrossRef] [PubMed] [Google Scholar]
- An evaluation of YEN and W angle in the assessment of anteroposterior jaw relationship. J Indian Orthod Soc. 2016;50:26-30.
- [CrossRef] [Google Scholar]
- Diagnostic validity of different cephalometric analyses for assessment of the sagittal skeletal pattern. Dental Press J Orthod. 2018;23:75-81.
- [CrossRef] [PubMed] [Google Scholar]
- MKG angle: A true marker for maxillomandibular discrepancy. J Indian Orthod Soc. 2020;54:220-5.
- [CrossRef] [Google Scholar]
- W angle: Sagittal jaw dysplasia indicator for orthodontic diagnosis outcome. J Med Sci Clin Res. 2019;7:61-6.
- [CrossRef] [Google Scholar]
- Tau angle: A new approach for assessment of true sagittal maxillomandibular relationship. Int J Clin Pediatr Dent. 2020;13:497-500.
- [CrossRef] [PubMed] [Google Scholar]




